
The lower lip is controlled by four key muscles—depressor labii inferioris (DLI), depressor anguli oris (DAO), mentalis, and platysma—working together under the direction of the facial nerve. These muscles and their nerve supply play a critical role in helping you smile, speak, eat, and communicate emotion in ways so automatic you never think about them… and they lie directly within the surgical field of procedures like facelift, neck lift, and synkinesis surgery.
That overlap is not a coincidence. It is exactly why understanding lower lip anatomy is essential for surgical safety and natural-looking results.
Our new study — published in Plastic and Reconstructive Surgery — takes the most rigorous look to date at which facial nerve branches control lower lip movement in living patients. Our findings challenge decades of textbook assumptions about facial nerve anatomy and have direct implications for surgical safety, leading us to change how we approach face and neck surgery in our own practice.
What Muscles Control the Lower Lip?
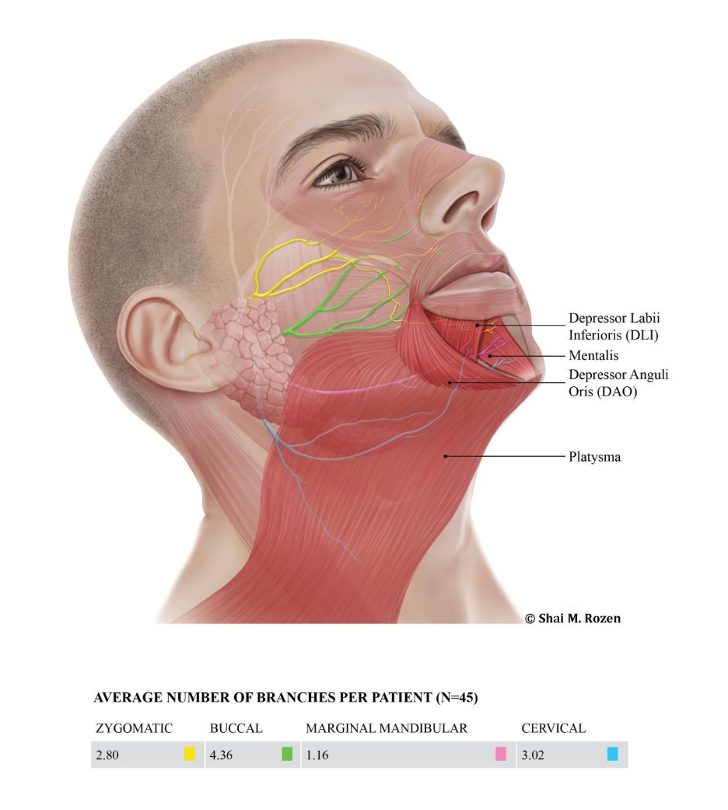
The lower lip is controlled by four muscles—the depressor labii inferioris, depressor anguli oris, mentalis, and platysma—which work together to control movement, expression, and symmetry.
- Depressor labii inferioris (DLI) — pulls the mid lower lip downward and slightly to the side, essential for the natural movement of smiling and speaking
- Depressor anguli oris (DAO) — depresses the corner of the mouth, contributing to expressions of sorrow or displeasure
- Mentalis — elevates the lower lip and chin, creating chin dimpling
- Platysma — tightens the neck and contributes variably to lower lip depression
Each of these muscles is innervated by branches of the facial nerve—but the specific branches that supply them, and in what proportion, had never been definitively established through functional, in vivo testing in live patients. Most prior research relied on cadaveric dissections, which can map anatomy but cannot tell you which nerve actually activates each muscle during real facial movement.
How Did We Conduct the Study—and Why Does It Matter for Facial Nerve Surgery?
Our study included 45 patients with facial synkinesis who underwent selective neurectomies and selective myectomies in our practice. The study used real-time, intraoperative nerve mapping, providing more accurate, functional data than traditional cadaver-based research.
How we mapped facial nerve function during surgery
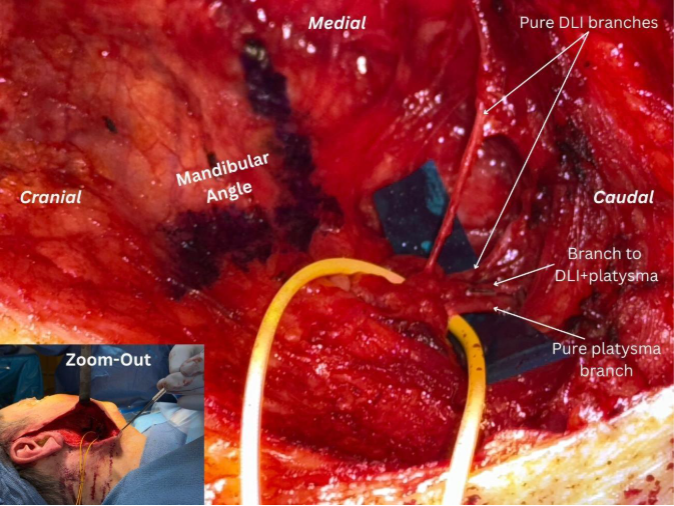
During surgery, we routinely and systematically dissected and stimulated each facial nerve branch using a nerve stimulator to precisely record which muscle each branch activates. This approach supports safe, accurate decision-making during surgery and provides granular, functional data at a scale not previously reported.
What we found: consistent patterns with clinical impact
The findings were highly consistent across all 45 patients, and the branch patterns we identified in this cohort are in line with our experience dissecting facial nerve branches in healthy individuals during cross-facial nerve graft procedures. Unlike prior cadaveric studies, which suggested the marginal mandibular nerve (MMn) was the primary driver of lower lip depression, our live functional data demonstrate a meaningfully different, clinically relevant pattern of innervation.
Which Nerve Controls the Lower Lip? Key Findings From Our Study
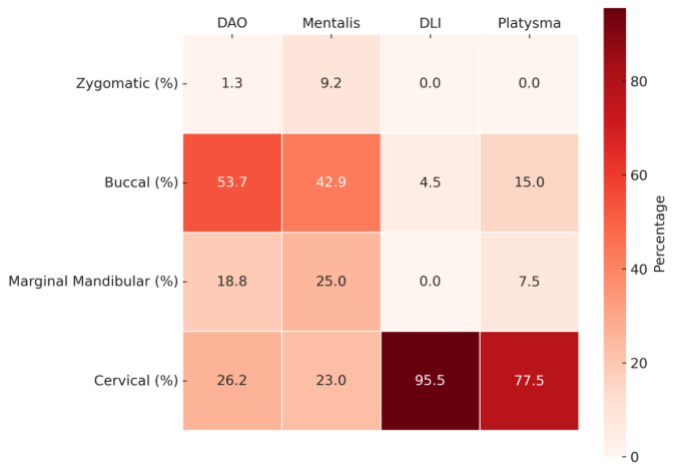
The most significant finding of this study is that the depressor labii inferioris (DLI)—the primary muscle responsible for lowering the mid-lower lip—is predominantly controlled by cervical branches of the facial nerve, rather than the marginal mandibular nerve (MMn) as traditionally taught.
For decades, the textbook teaching held that the marginal mandibular nerve (MMn) was the primary innervator of the DLI. However, our intraoperative functional mapping found something different:
- 95.5% of nerve branches supplying the DLI were cervical branches, not the MMn.
- Nearly 70% of those were pure DLI cervical branches, meaning they innervated only this muscle.
- The MMn played a less significant role in DLI activation than previously believed.
This represents a meaningful shift in our understanding of facial nerve anatomy, and it has direct implications for aesthetic facial plastic surgery and synkinesis surgery.
Why this matters for surgery?
The marginal mandibular nerve runs near the lower border of the jaw near the facial vessels—an area surgeons are appropriately cautious about during facelifts and neck dissections. In contrast, the cervical branches that control the DLI travel beneath the platysma, emerging from beneath the parotid tail approximately 1.5 cm below and behind the mandibular angle.
This anatomical pathway places these cervical branches at particular risk during specific facial plastic surgery procedures, particularly when the platysma is divided too high.
If these branches are inadvertently injured, the following risks may occur:
- The lower lip may elevate unnaturally
- Smile symmetry can be disrupted
- The result can be difficult to reverse
What Does This Mean for Facelift, Neck Lift, and Synkinesis Surgery?
This research shows that precise knowledge of facial nerve anatomy—especially the cervical branches that control the lower lip—is essential for avoiding complications and achieving natural-looking results in facelift, neck lift, and synkinesis surgery.
The significance of the platysma
The platysma is not just a reconstructive surgeon’s concern—it is central to aesthetic surgery of the face and neck. This muscle is routinely addressed during facelifts, neck lifts, and deep plane procedures, and it plays a key role in correcting visible neck banding that occurs with aging.
In my practice, I perform the same sub-SMAS dissection and platysma work in aesthetic patients as I do in facial paralysis and synkinesis surgery. The tissue planes are identical. The nerve branches are the same.
Where surgical risk occurs—and why technique matters
The risk is also the same: if the platysma myotomy is performed too high, without accounting for the cervical branches traveling along its undersurface—those nerves can be inadvertently injured. This can affect lower lip position and facial symmetry, regardless of whether the procedure is reconstructive or cosmetic.
As we have written previously, my experience performing close to a thousand facial palsy-related procedures directly informs every aesthetic case I perform, even when the goal is simply rejuvenation.
This new research reinforces the following critical principles:
- Facial nerve anatomy is complex and highly specific
- Redundancy between nerve branches is limited
- Even small variations in technique can have lasting functional consequences
Our data also provides a more precise surgical roadmap:
- The DLI cervical branch exits beneath the parotid tail
- It’s located approximately 1.5 cm below and behind the mandibular angle
This level of anatomical precision allows for safer surgical planning and more consistent preservation of natural lower lip movement.
Real Results: Improved Lower Lip Symmetry After Selective Neurectomy
The following two patients demonstrate that selective MMn neurectomy — with careful preservation of the cervical DLI branches — produces meaningful improvement in lower lip symmetry and function without any worsening of lower lip position.


What Questions Should You Ask Before Facelift, Neck Lift, and Synkinesis Surgery?
Before undergoing facelift, neck lift, or synkinesis surgery, you should ask your surgeon about how they protect facial nerve function—especially the branches that control lower lip movement and facial symmetry.
Here are the key questions to help you better understand your surgeon’s approach:
- How do you manage the platysma during neck surgery?
- What is your approach to identifying and protecting the facial nerve branches in the lower face and neck?
- How do you minimize the risk of affecting lower lip movement or smile symmetry?
- If a facial nerve injury occurs, what treatment or reconstruction options are available?
These are not “gotcha” questions—they are the kinds of questions that reflect the complexity of surgery in this region, and any leading facial paralysis surgeon and board-certified plastic surgeon should welcome them.
Final Thoughts: Why Lower Lip Anatomy Matters for Safe, Natural Results
The lower lip may be small in surface area, but it plays a large role in facial expression, communication, and identity—and the nerves that control it must be preserved to maintain natural movement and symmetry.
The nerves that move the lower lip are anatomically consistent enough that we can now map them with confidence—and surgically specific enough that an error of a centimeter or two in technique can mean a complication that alters a patient’s smile for life. Our study findings reinforce that lower lip function depends on precise nerve anatomy, particularly the cervical branches of the facial nerve, and that this knowledge directly informs safer, more accurate facelift, neck lift, and synkinesis surgery.
Our group has dedicated significant effort to understanding this anatomy at the level it deserves, and this study represents a new standard of functional evidence in that effort. I am grateful to my co-authors Lior Har-Shai, Christine Johansen, and Sahejbir Bhatia for the meticulous work that made it possible.
Here For You
Remember, we’re here to guide you through your aesthetic facial and reconstructive options with expertise and care. Explore your options by using our online form to request a consultation or call us at (214) 645-2353.
The full study — “Muscles of the Lower Lip: Functional Anatomy, Innervation Patterns, and Nerve Injury Prevention” — is published in Plastic and Reconstructive Surgery and is available at DOI: 10.1097/PRS.0000000000012836 (abstract on PubMed).
— Dr. Shai M. Rozen, Board-Certified Plastic Surgeon, Professor and Vice-Chair of Plastic Surgery, University of Texas Southwestern Medical Center
Leave a Reply