
Perhaps the highest priority in treating patients with facial paralysis is preventing blindness. The cornea is a thin layer of tissue that covers the pupil that is crucial for allowing light to enter the eye and reach the retina, thus allowing vision. Protection of the cornea is crucial because injury to the cornea may eventually result in blindness. Luckily, the cornea heals well. If the cornea is protected with appropriate lubrication and the patient can close the upper and lower eyelid during the daytime and nighttime, the cornea has a chance to stay healthy and recover efficiently from injury.
What Can Injure the Cornea?
Due to injury of the facial nerve, facial palsy patients lose many of the following protective mechanisms, including:
- The lacrimal gland loses its capacity to produce tears resulting in a constantly dry eye.
- Paralysis of the orbicularis oculi muscle that surrounds the eye creates the inability to close the upper eyelid during the day (mostly blinking) and at night (this is termed paralytic lagophthalmos).
- The lower eyelid droops from its normal position and becomes lower than the one on the uninjured side, a phenomenon termed ectropion, which decreases coverage of the lower part of the eyeball.
When all of these deficiencies occur, the cornea is less protected, increasing the risk of corneal injury and eventual blindness.
Non-Surgical Eye Protection Treatments
The initial treatment objective is immediate protection of the cornea using eyedrops during the day and ointment or a moisture chamber (covering the eye with a specialized patch) at night. Because some patients subsequently recover from their facial paralysis to different degrees and do not need surgery, if there is a chance for recovery, surgery is often not the first treatment choice. Only experienced surgeons with in-depth knowledge of the facial nerve can assess whether early surgical intervention is warranted versus waiting for recovery while protecting the eye with the aforementioned non-surgical means. (Learn more about surgical and nonsurgical treatments for protecting the eye.)
Surgical Eye Protection Options
Patients who do not improve or have little chance of improvement require longer-term surgical solutions. Traditionally, we use an upper eyelid weight to help the upper eyelid close and surgically lift the lower lid. We modified both techniques, the upper eyelid weight in 2013 and the lower eyelid procedure in 2022, and they were published in the most important journal in the field of plastic surgery – The Journal of Plastic and Reconstructive Surgery. These procedures will be detailed in Part 2 of this blog post.
But perhaps most important is the research published in 2021 on the value of innervating the orbicularis oculi muscle surrounding the eye in facial paralysis patients who were seen by us early enough (within around 18 months of their paralysis). When patients do not show recovery of their facial nerve, the objective is to re-innervate their facial (mimetic) muscles, including the orbicularis oculi muscle around the eye. We do this with microsurgical techniques while recruiting healthy nerves to innervate the injured facial nerve (think of it as rewiring).
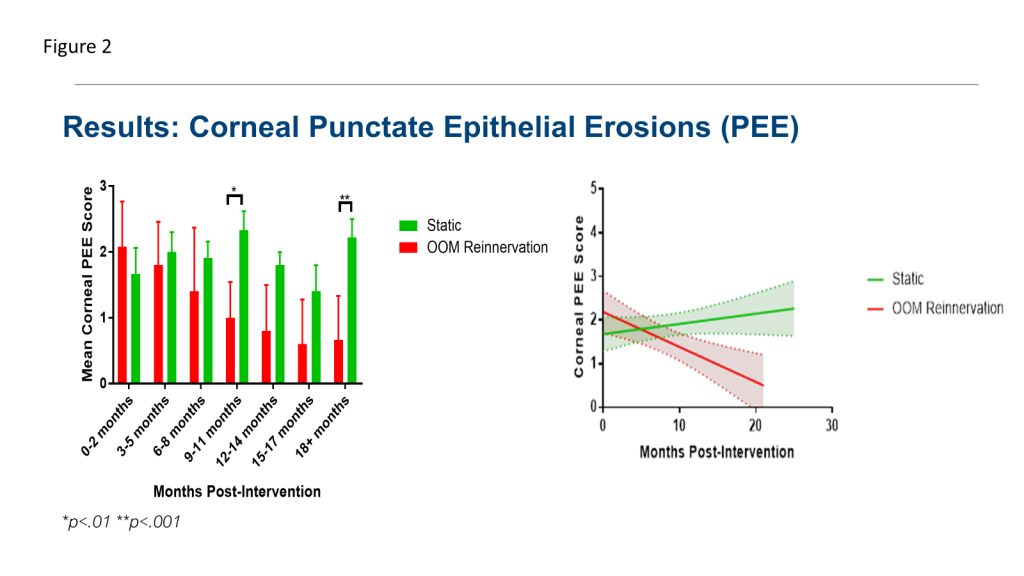
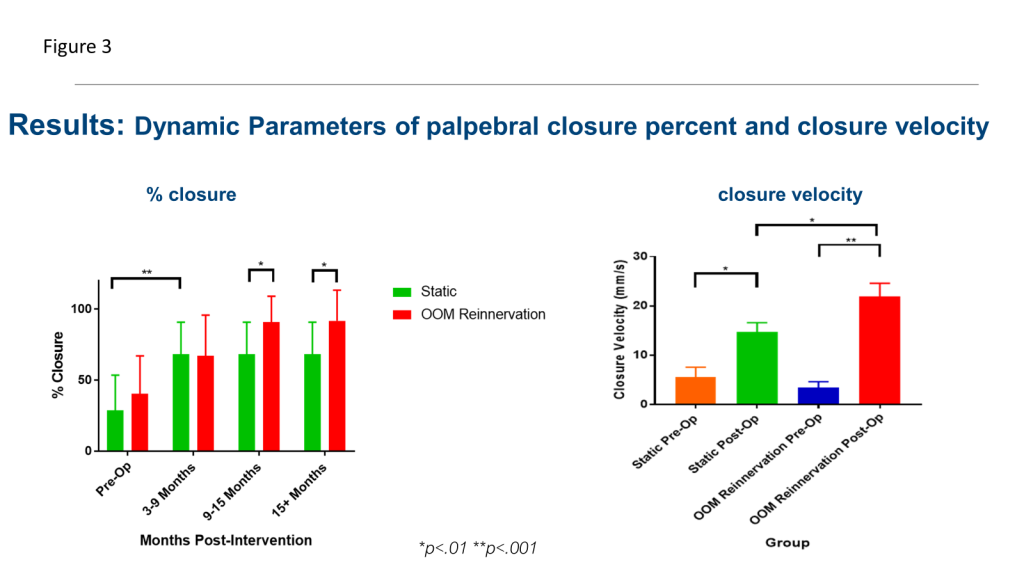
When we compared two groups of patients, those whose surgery involved an upper eyelid weight and lower eyelid support versus those who underwent the same procedures with the addition of re-innervating the muscles around the eye, the results were astonishing. The patients who came to us early enough to undergo re-innervation had significantly less corneal injury than the ones who did not undergo re-innervation surgery. Additionally, the percentage of eye closure and speed of eye closure were significantly improved in the re-innervation group. This emphasized the importance of early intervention via re-innervation techniques. For a visual, see Figures 1, 2, and 3.
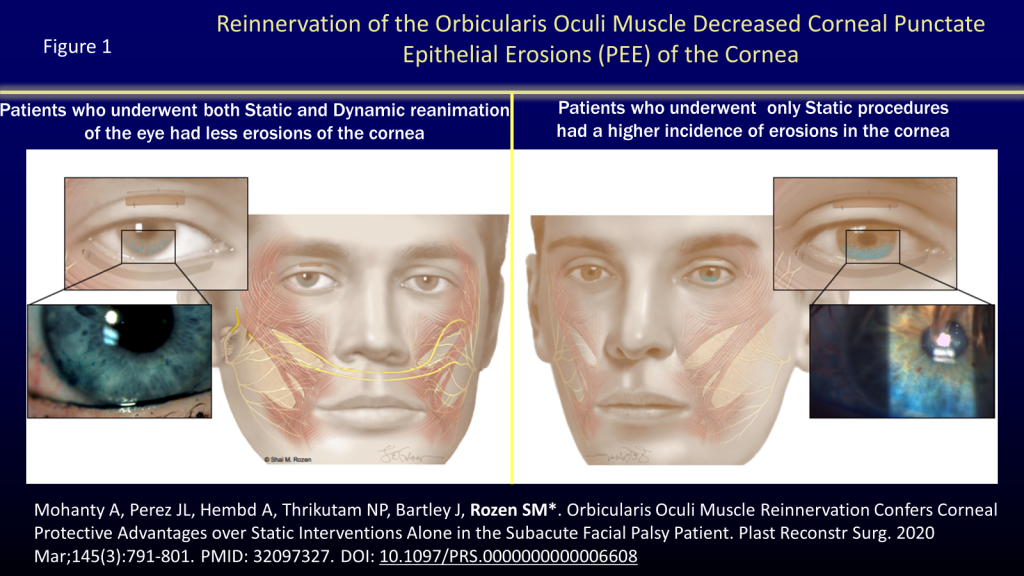
For in-depth reading about re-innervation or the muscles around the eye, we provided you with a link to the abstract (Mohanty A, Perez JL, Hembd A, Thrikutam NP, Bartley J, Rozen SM*. Orbicularis Oculi Muscle Reinnervation Confers Corneal Protective Advantages over Static Interventions Alone in the Subacute Facial Palsy Patient. Plast Reconstr Surg. 2020 Mar;145(3):791-801. PMID: 32097327. DOI: 10.1097/PRS.0000000000006608)
Hopefully, this blog post provides you with a helpful glimpse into our considerations of how to protect the eye via re-innervations techniques.
For more about upper and lower eyelid procedures to protect the eye, please see Part 2 of this blog post.
Leave a Reply