
Why Won’t My Lip Go Down on the Side That I Have Synkinesis?
As mentioned in previous blogs on synkinesis, one of the characteristic findings is that certain muscle groups work against each other rather than working in synchrony. A simple example of this is the activity of the biceps and triceps muscles in the arm. When we try to lift a weight, our biceps muscle flexes, and our triceps muscle (the back muscle of the arm) relaxes simultaneously. But if, for some reason, the triceps muscle contracts at the same time as the biceps muscle contracts, lifting the weight would not be possible since the arm and forearm would be “frozen,” in other words, exerting equal forces in opposite directions. This is what commonly occurs in the face when synkinesis occurs.
We’ve understood this phenomenon for years, and a good example of this is the antagonistic effect the depressor anguli oris muscle has on the corner of the mouth, pulling it down against the lifting activity of another muscle, called the zygomaticus major. This, in effect, inhibits the raising of the corner of the mouth. Once we weaken the abnormal co-contraction of the depressor anguli muscle—either by selective myectomy or selective neurectomies—patients are more capable of smiling and often have improved speech and oral and lip control, as seen in Figure 1.

Figure 1. A: Before a Depressor Anguli Oris Myectomy

Figure 1. B: After a Depressor Anguli Oris Myectomy
The Lower Lip
Still, one of the main unsolved problems was the lower lip in patients with synkinesis. Although we often improved the patient’s ability to smile, the lower lip on the synkinetic side would remain elevated, often covering the lower and even upper teeth, creating significant asymmetry and sometimes even resulting in patients biting their lower lip.
For many years, we thought this was due to weakness or paralysis of the depressor labi inferioris muscle. This muscle depresses the lip in a location slightly more central (medial) than the depressor anguli oris muscle that pulls down the corner of the lip (the oral commissure). This line of thinking that the depressor labi inferioris muscle was weak in synkinetic patients diverted our attention from what is perhaps the most common cause of abnormal lower lip elevation in synkinetic patients: the very hyperactive and strong mentalis muscle which forces the lip upwards by overcoming the natural downward pull of the depressor labi inferioris, as seen in the patient in Figure 2.
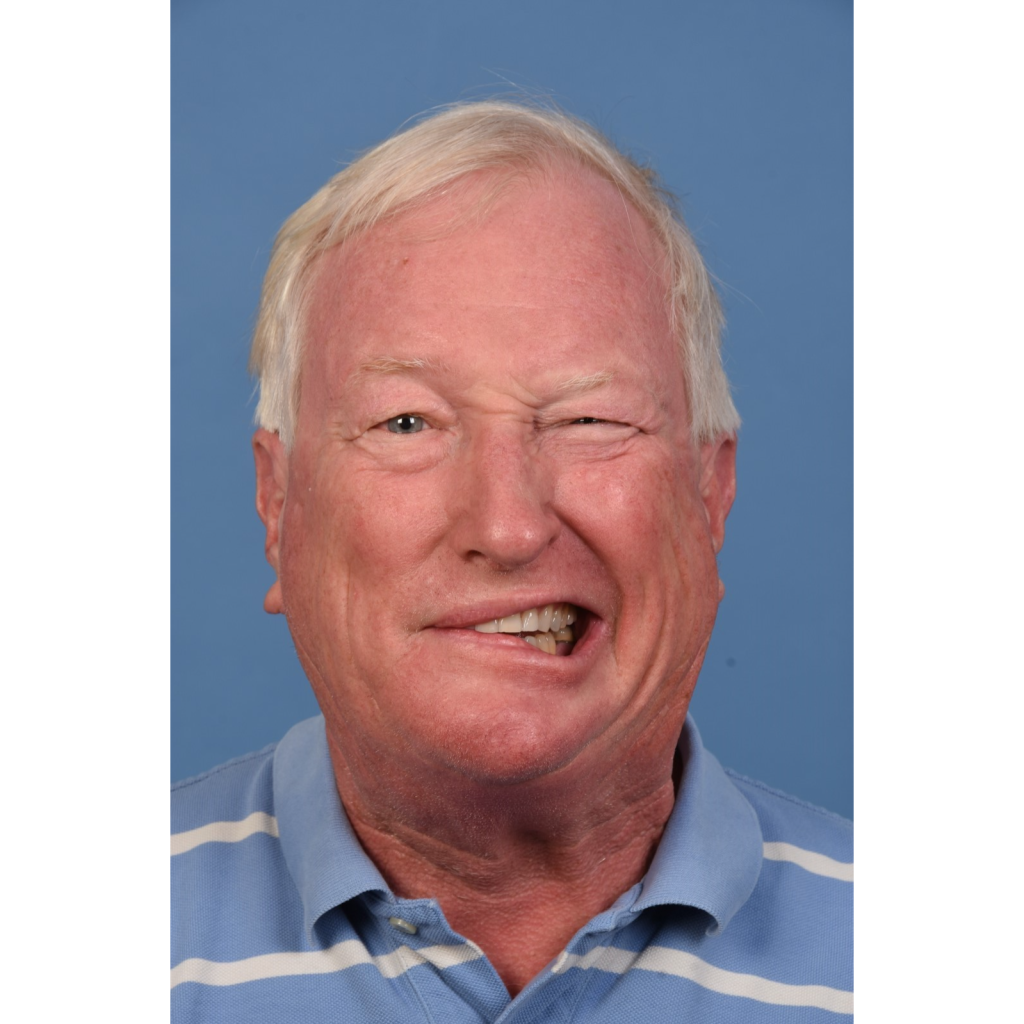
Figure 2: Patient with synkinesis and elevated right lower lip due to mentalis muscle hyperactivity.
The Solution: Weakening the Mentalis Muscle
After research was performed on the nerve pathways and the innervation patterns of the different muscles surrounding the mouth, our group started implementing these findings into surgical practice. Rather than attempting to strengthen the depressor labii inferioris muscle as previously thought, the goal was to weaken the mentalis muscle, which was too strong and forced the lips upward.
This resulted in significant improvements in the care of patients with synkinesis, with marked improvement in results, as seen in Figures 3 and 4. The previously high lower lip would now be much closer to a normal position. For this finding, Dr. Rozen’s research group received a best paper award at the 2024 annual meeting of the American Society for Reconstructive Microsurgery and was later published in the Journal of Plastic and Reconstructive Surgery.


Figure 3. A: Patient who had Bell’s Palsy and developed synkinesis (before treatment)
Figure 3. B: After depressor anguli oris selective myectomy and selective neurectomies targeting the mentalis muscle.
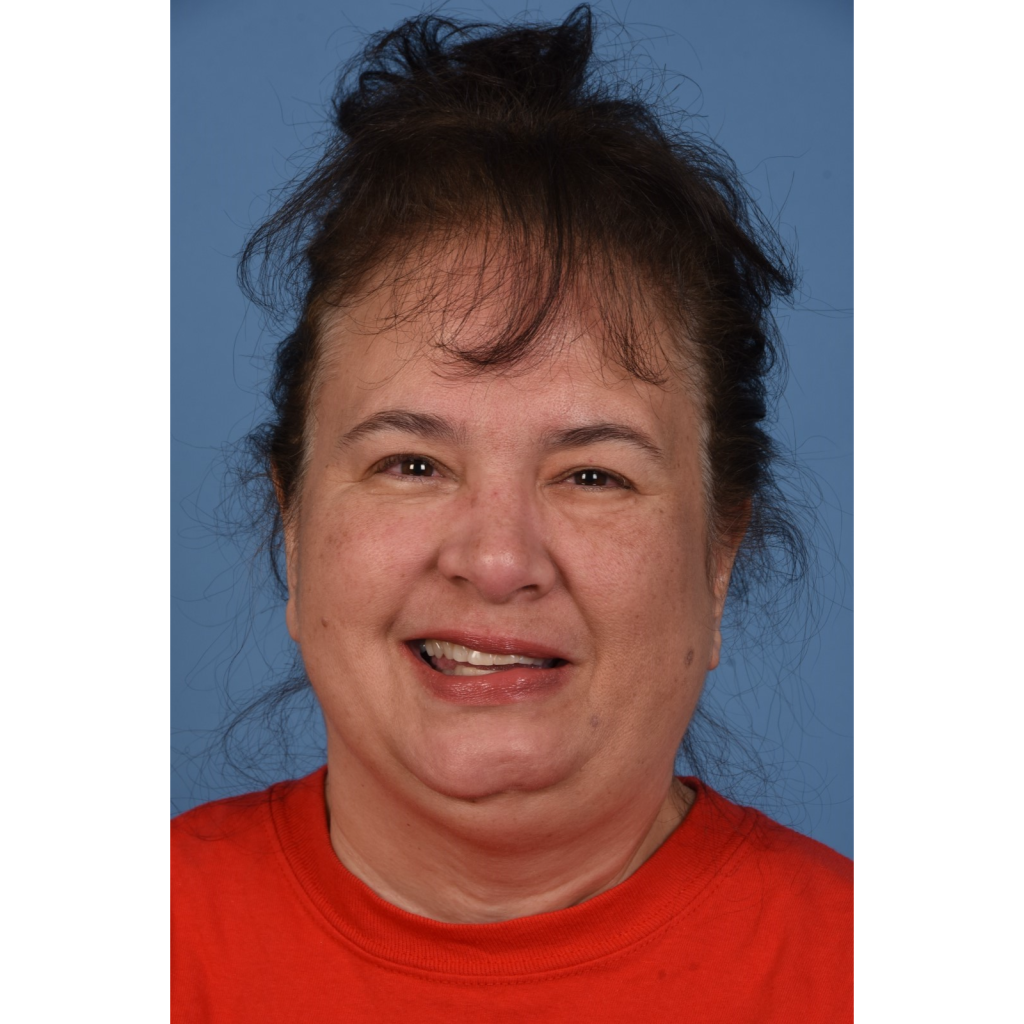
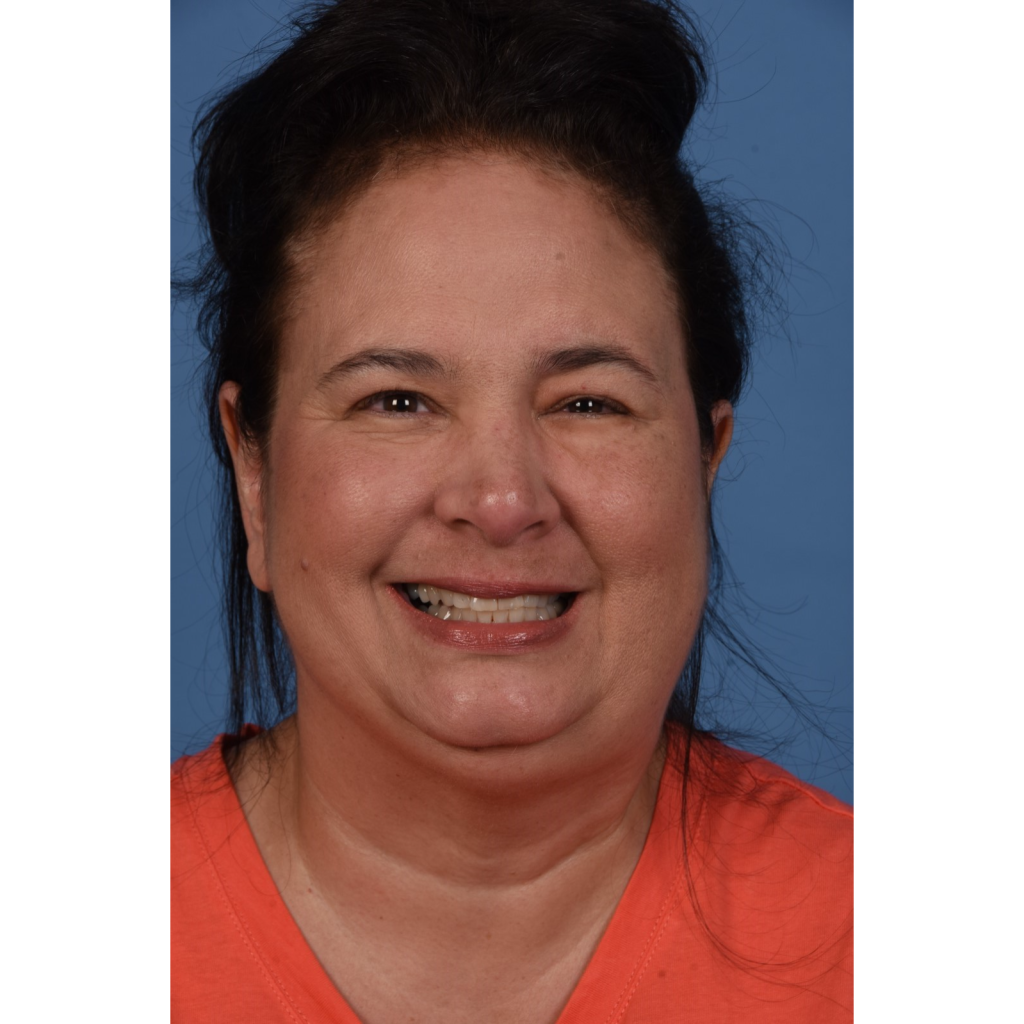
Figure 4. A: Patient who had Ramsay Hunt Syndrome and developed synkinesis
Figure 4. B: After depressor anguli oris selective myectomy and selective neurectomies targeting the mentalis muscle.
How Do I Know if My Mentalis Muscle Is Causing My Lower Lip To Stay High?
If you have complete flaccid (no motion and tone at all) facial paralysis, then the lower lip does not pull down because of a paralyzed depressor labii inferioris muscle- not because of a hyperactive mentalis. If you partially recovered and have synkinesis, then dimpling of the chin may suggest an overactive mentalis muscle, and exploring the option of weakening it may be worthwhile during the discussion with a specialist.
How We Improve the Lower Lip Position in Synkinesis
In order to weaken the mentalis muscle, two approaches can be taken:
- Selective myectomy of the mentalis muscle, OR
- Selective neurectomy of the nerves innervating the mentalis muscle
Our current approach is to weaken the mentalis muscle through selective neurectomies for the depressor labii inferioris muscle and selective myectomy for the depressor anguli oris muscle, such as in the patient in Figure 4.
We prefer this approach in most patients since: (1) We are already performing selective neurectomies, and this would be simply an extension of that procedure, and (2) We can avoid a potential contour deformity if we were to remove the muscle.
In summary, in patients with synkinesis, a common reason for the lower lip staying high and not depressing equally to the lower lip on the other side is a hyperactive mentalis muscle, which overpowers the lower lip depressor muscle (the depressor labii inferioris muscle). By weakening this muscle through selective neurectomy, we may obtain improved symmetry, oral function, and speech and possibly decrease lip biting.
You can read more about synkinesis treatments in our related blog post. If you want to discuss your treatment options, please request a consultation or call us at (214) 645-2353 to get started.
Leave a Reply